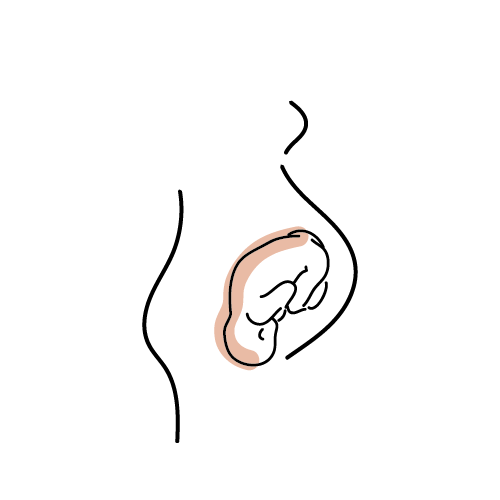
Due to the shape of the head when in the posterior position, this can prevent the ability for bubs head to be able to enter the pelvis and ‘sit’ on the cervix to help stimulate labour. This is the normal physiological process to birth a posterior baby vaginally. Hold trust in your body, and trust in the process.
- Rupture of membranes before labour
- Long start-stop pre-labour phase (often called spurious labour)
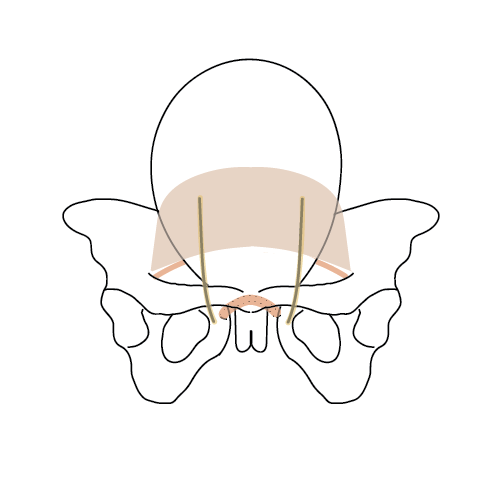
This is a natural physiological process that babies in OP position need to have a functional, vaginal birth. Once again hold trust in your body, and trust in the process. As long as your ligaments are balanced the position your baby is in right now is the RIGHT position for your body, pelvis and baby.
Normal, normal, normal. This is what your body and baby needs to birth a posterior baby vaginally.
As above
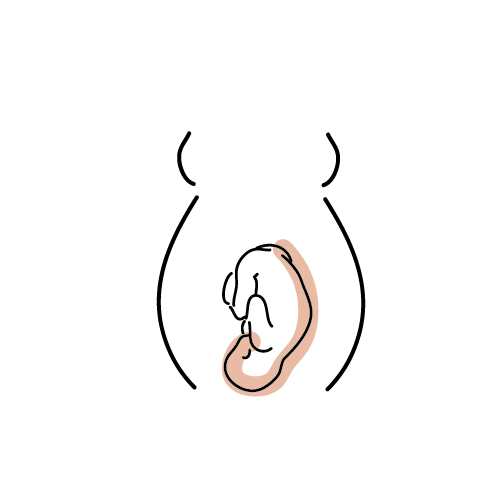
The urge to push is created when the hard surface of babies head descends into the pelvis enough to put pressure on the rectum & pelvic floor through the vaginal wall. This early pushing urge happens in 20%-40% of vaginal births and 41% of babies in an OP position.